The LSEQ is the most popular measure for psychopharmacological research into subjective aspects of sleep throughout the world.

Description
The Leeds Sleep Evaluation Questionnaire (LSEQ) was designed to measure the self-reported effects of psychoactive drugs on sleep and awakening (Hindmarch, 1975).
It has been employed in numerous psychopharmacology studies, in single and repeated dose studies, with both patients and volunteers, involving over 50 psychoactive compounds, including benzodiazepine and non-benzodiazepine sedative-hypnotics, antidepressants, CNS stimulants, and many other types of drug.
The widespread usage and enduring popularity of the LSEQ reflects various factors. Its simplicity and brevity mean that it is well accepted by both patients and volunteers, while the visual analogue responses are easy to score and analyse. The absence of learning or fatigue effects make it particularly suitable for repeated measure studies. In psychometric terms it demonstrates both sensitivity and reliability, and it has high construct validity with objective sleep indices.
Yet despite the structural simplicity and brevity of the LSEQ, it still manages to provide full coverage of all the basic aspects of sleep. Devine et al (2005) undertook a ‘Systematic review of patient-reported outcome instruments measuring sleep dysfunction’. Twenty two measures emerged from their initial literature review, but only six were found to cover the target sleep domains – which had been selected a priori. Included in this list of the top six was the Leeds Sleep Evaluation Questionnaire
The list of psychoactive drugs assessed using the LSEQ is available HERE. Psychoactive drugs assessed using LSEQ
In 2016, Prof. Hindmarch passed the academic/scientific oversight of the LSEQ to Dr. Neil Stanley.
The LSEQ was designed to measure the self-reported effects of psychoactive drugs on sleep and awakening.
Conceptual Origins
The LSEQ was initially developed specifically to measure the effects of sedative-hypnotic drugs such as the benzodiazepine derivative temazepam (Hindmarch, 1975). After two initial pilot studies, the final version of questionnaire was decided; it was termed the ‘Sleep Evaluation Questionnaire’. Further details of this early period in the development of the LSEQ, and of the other subjective sleep questionnaires then available, are described in Parrott and Hindmarch (1978).
Psychometric analysis of these early studies demonstrated that the LSEQ displayed psychometric reliability and sensitivity to psychoactive drug effects (Parrott and Hindmarch, 1978); so that the basic format of the questionnaire has remained unchanged to this day. The only slight modification was an expansion of title into ‘The Leeds Sleep Evaluation Questionnaire’.
The first four published studies with the LSEQ involved acute and chronic dosing regimens of 1,4-benzodiapepine derivates such as temazepam, nitrazepam and flunitrazepam, and the 1,5 benzodiazepine derivative clobazam (Hindmarch, 1975; Hindmarch et al, 1977; Hindmarch and Parrott, 1977). The combined data from all these studies was analyzed using a series of factor analyses (Parrott and Hindmarch, 1978). They confirmed the four factors around which the questionnaire had been designed: getting to sleep, quality of sleep, awakening from sleep, and behaviour following wakefulness (Figure 1). Oblique final rotation showed that the two sleeping state factors were positively correlated (GTS with QOS), and the two waking state factors correlated together (AFS with BFW), but that the sleeping and awakening states were basically orthogonal or independent. This same factor structure emerged in the overall analysis, when the active drug conditions were analyzed alone, and when the placebo data was analyzed separately (Table 1 in Parrott and Hindmarch, 1978).
The next few years saw a number of further studies into other sedative hypnotics, along with dose-ranging studies of temazepam and clobazam, and a number of studies involved drug combinations, such as clobazam with nomifensine (Parrott et al, 1982; Stonier et al, 1982).
Another area of research involved the assessment of drugs where sedation was an undesirable side-effect. Antihistamines are often used as a daytime medication for disorders such as allergic rhinitis or ‘hay fever’ (Parrott, 1987). The first clinically available antihistamines such as promethazine induced feelings of daytime drowsiness (Hindmarch and Parrott, 1978a), and impaired cognitive task performance (Hindmarch, 1976; Parrott and Wesnes, 1987). These characteristics made then unsuitable for use by patients needing to drive cars or heavy goods vehicles, or operating industrial machinery, where sedation would increase the risk of accidents (Hindmarch, 1976; Parrott, 1987; Parrott et al, 2004). Pharmaceutical companies were therefore developing peripherally active antihistamines, without central nervous system sedation. Studies with the LSEQ confirmed that newer compounds such as clemastine and mebhydrolin, did not affect subjective aspects of sleep, whereas earlier drugs such as promethazine led to significant sedation (Hindmarch and Parrott, 1978). This confirmed the practical advantages of the more modern antihistamines as daytime medications (Hindmarch, 1976). The LSEQ was also found to be sensitive to the effects of CNS stimulants such an amphetamine, which impaired the ease of getting to sleep, reduced the quality of sleep, but facilitated morning awakening (Parrott et al, 1980). These and other studies were summarized in the first empirical and theoretical review of the questionnaire, which concluded that it was a sensitive and reliable measure for many different types of psychoactive drug, in addition to sedative hypnotics (Parrott and Hindmarch, 1980).
The LSEQ has been translated into more than 40 language versions. The work of forward and backward translating the LSEQ in this multitude of languages was carried out by Mapi Language Services (including seemingly separate versions in French and Belgian French).
Over the years the LSEQ remained essentially the same. Cronbach’s alpha and Pearson’s r correlations continued to confirm the questionnaires internal consistency, even when used cross-culturally (Tarrasch et al 2003) and studies continued to demonstrate the questionnaire’s usefulness and consistency across age ranges (Hindmarch et al 2000; Tarrasch et al 2003). It continued to be used as a reliable and valid tool for the measurement of the sedative effects of drugs ranging from caffeine (Hindmarch et al 2000) to milnaciprane (Hindmarch et al 2000). It also remained at the fore of studies investigating quality of sleep, whether this involved normobaric tents (Pedlar et al 2005) or the assessment of the hypnotic efficacy of new or modified compounds (Hindmarch et al 2006).
Zisapel and Lauden (2003) undertook a very detailed and comprehensive review of the LSEQ. They summarized the findings from 83 peer reviewed papers involving around 38 different psychoactive compounds, which included 14 benzodiazepine derivatives, 2 non-benzodiazepine sedative hypnotics, 14 antidepressants, 5 antihistamines, 3 anxiolytics (see Table 1). This latter table also includes data from several 2004-2007 studies which involved previously unstudied compounds. Treatment effects on the LSEQ correspond to those found with other measures of hypnotic drug effects, both objective and subjective (sleep diaries) and the BFW component reflects that shown using tests of daytime vigilance. The studies reviewed also show that not only can the LSEQ measure the direct effects of drugs on sleep but also the improvement in sleep caused by the amelioration of depressive symptoms with treatment. The LSEQ is shown to be able to discriminate dose and time effects of drugs. The review concludes that the LSEQ is “a psychometrically sound measure of sleep latency and quality as well of ‘hangover effects’ predominately in insomnia” and the data presented supports the use of the LSEQ in a variety of clinical populations (adults/elderly, depressed/insomnia patients).
The enduring utility of the Leeds Sleep Evaluation Questionnaire is a reflection of several qualities. It is brief, clear and simple to complete, with a high level of face validity (Parrott, 1991). Its brevity also makes it easy to complete, so that it is well-received by patients and volunteers, even for participants at the lower end of the IQ spectrum. Since there are few learning or training effects, this means that practice and/or fatigue does not interfere with drug effects. The best questionnaires are simple and focused, since they provide clear answers to well-defined questions.
Conditions of Use and Available Translations
The LSEQ is distributed by Mapi Research Trust on behalf of its copyright holder, Prof. Ian Hindmarch.
Mapi Research Trust is a non-profit organization dedicated to improving patients’ quality of life by facilitating access to Clinical Outcomes Assessments (COAs) information by centralizing information. Please visit Mapi Research Trust’s website for more information!
Any questions on the LSEQ, on its conditions of use, its available translations… shall be directed to Mapi Research Trust.
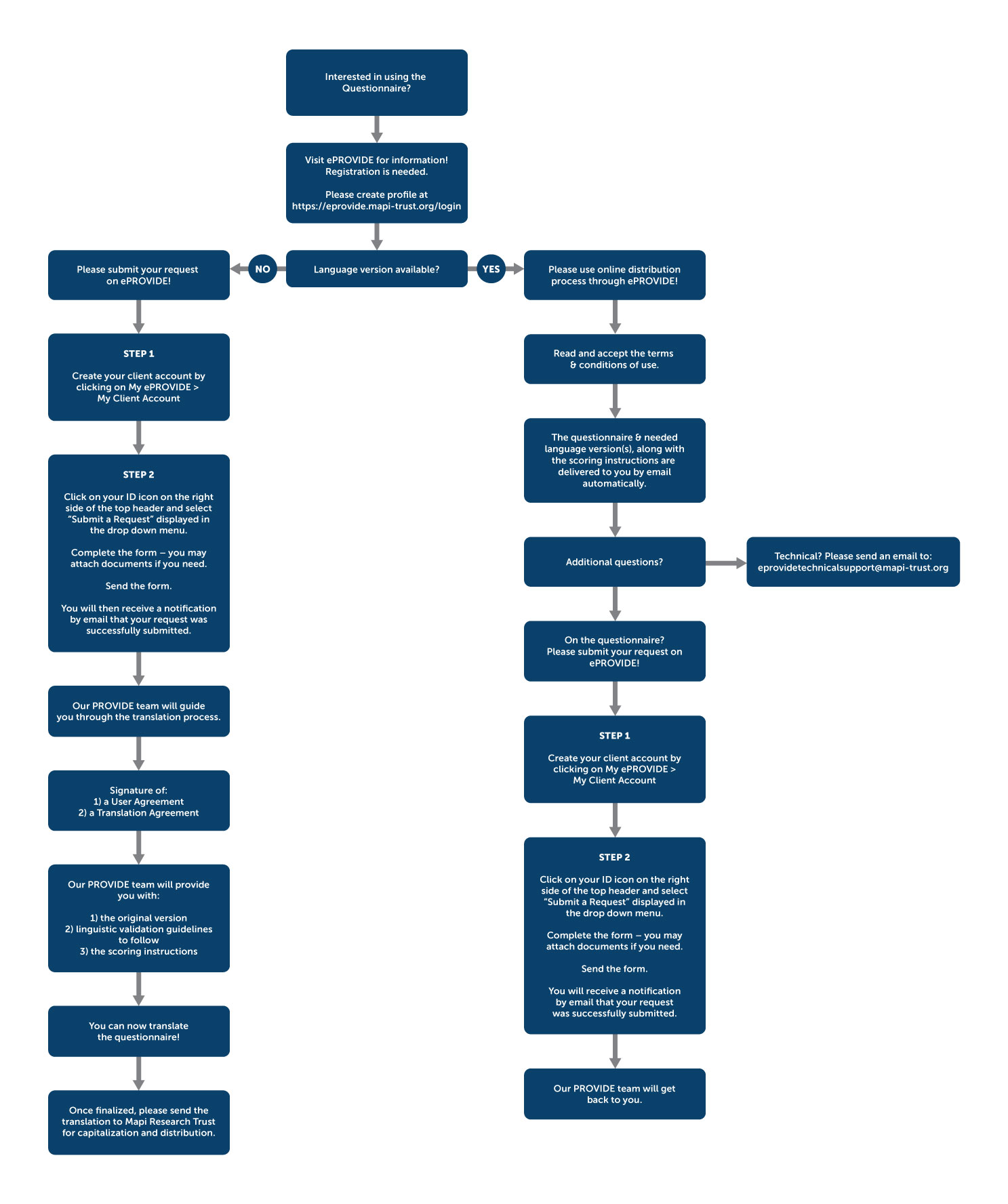
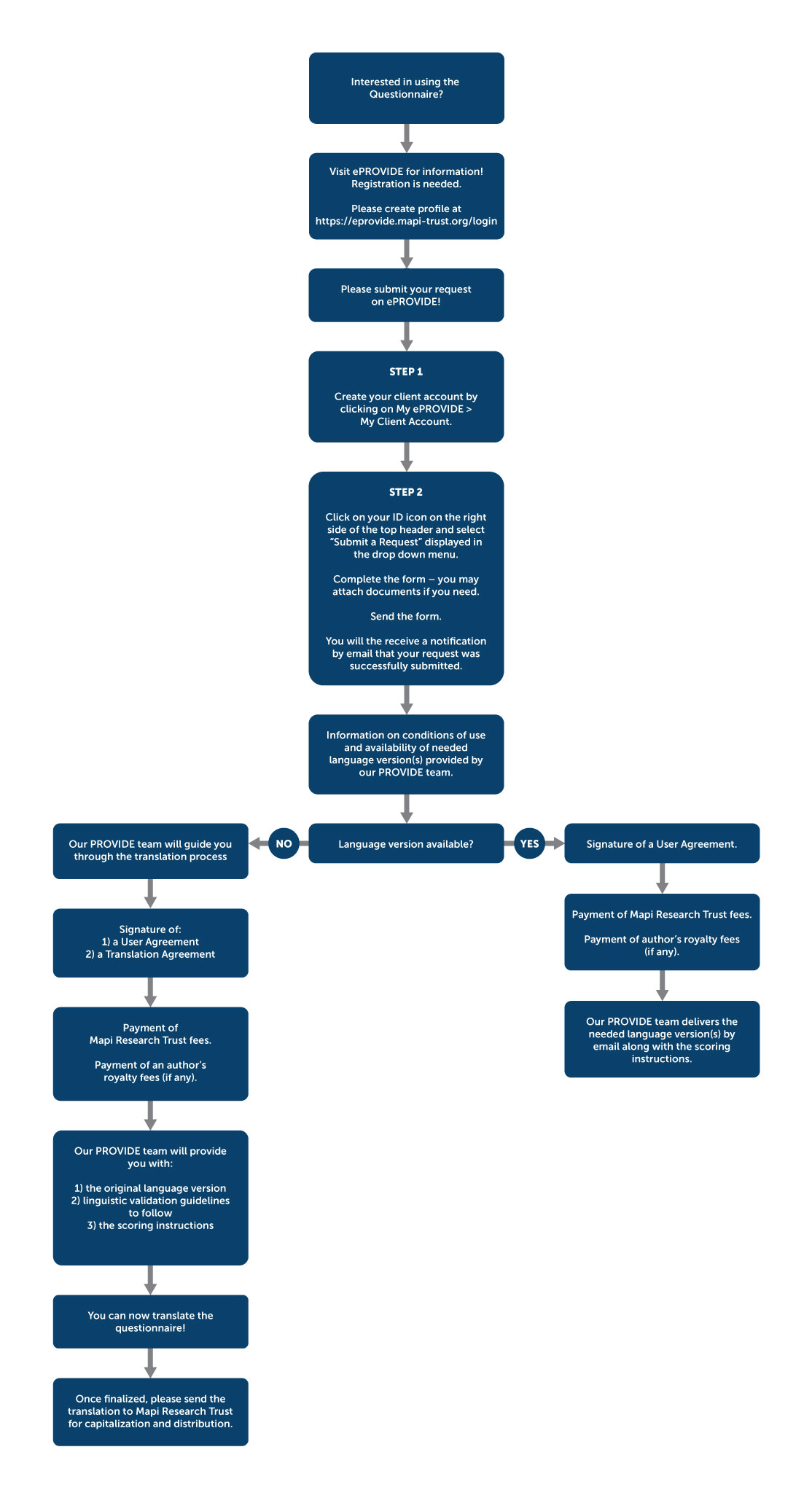
Please submit your request directly into our ePROVIDE™ database and our PROVIDE™ team will get back to you as soon as possible!
The list of existing and available translations of the LSEQ is available on ePROVIDE™.
Please see the detailed workflow for your request, whether you are
{kind=link}
{kind=link}
{kind=link}
Research Publications
a. Development and Validation
Parrott AC, Hindmarch I. Factor analysis of a sleep evaluation questionnaire. Psychol Med. 1978 May;8(2):325-9
Hindmarch I. 1,4 benzodiazepine, temazepam (K 3917), its effect on some psychological parameters of sleep and behaviour. Arzneimittel-Forschung (Drug Research). 1975;25(11):1836-1839
b. Other Publications Using The Questionnaire
Please click on this link Leeds Sleep Evaluation Questionnaire References to access additional bibliographic references or visit ePROVIDE™
The LSEQ is brief, clear, and simple to complete, with a high level of face validity.
Webinar on the LSEQ
Webinar on the Leeds Sleep Evaluation Questionnaire with Dr. Neil Stanley
Recorded session available here!
Prof. Ian Hindmarch, BSc, PhD, CPsychol, FBPsS, FFPM, FRSA

Emeritus Professor of Human Psychopharmacology, University of Surrey
Professor Ian Hindmarch joined to the academic staff of the University of Leeds in 1966 where he established the Human Psychopharmacology Research Unit (HPRU) in 1980. In 1990, he became Professor of Human Psychopharmacology and Head of the HPRU Medical Research Centre at the University of Surrey, where he remained until his retirement in 2005.His research concentrated in establishing, in volunteers and patients, the human psychopharmacological profile of the effects of psychoactive drugs on cognition, psychomotor function and the performance of the tasks of everyday living. His research has investigated the effects of antidepressants, hypnotics, anti-anxiety agents, antihistamines and cognitive enhancers as well as social drugs, alcohol and drugs of abuse. The results of his research appeared in over 600 medical and scientific publications, including books, monographs and journal supplements.
Contact Us
Please contact our PROVIDE™ team for any questions on the LSEQ:
Mapi Research Trust
PROVIDE™
27 rue de la Villette
69003 Lyon
France
Telephone: +33 (0)4 72 13 65 75